"The dangers of ORAL only cycles"
There's a NEW concept of running orals only, on for a few days, switch oral to an other, and switch those, in a repeated interval. (based off an old-school protocol of orals only) Let me explain the hazarded and the potentials for failed results and unwanted side effects.
Here you will read some info I have put together 80% of the read, and some other info I have shared, A mix of feedback and input that explains the hazard and do's and don'ts.. After hearing about oral only cycles and switching orals up every few day , here's my take in the instance
Let's talk a bout the "theory" orals off an on.. I'll begin with an opening statement by saying it's simply lousy and ineffective with everything that its attempting to be achieved..Oral hormones need to build a concentration in plasma,serum in the blood,this plasma in the blood medium provides information to other cellular groups that assist with enhancing and improving the drugs effectiveness and efficacy..This is why most (short half life drugs) inherent a protocol for its best advantage, there lets interpenetrate the results "steady,positive blood plasma, expressing optimal drug performance"
Now, you're gonna hear mix reviews on this supported with "regurgitated bro-science" all the while with no actual clinical data citing this to be effective. However, I have seen enough evidence that supports AAS having,creating a environment/platform with needs to have a steady on set/supply to remain effective..Each drug here in questions has a different course of action, half-life, plasma blood build-up etc etc, and each one independently and will imitate different metabolites and enzymes as they share different molecular and chemical structures/rational design and unique functionalities..
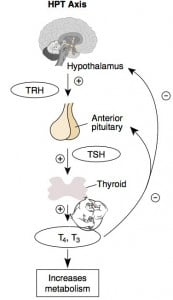
With this said: Now lets also take into great consideration AR upregulation with the presence of androgens, more AR sites throughout targeting tissue and these medications in the action in which is desired by the used..,There's a vast amount of activity in which a complex interplay between activation and inactivation mechanisms and signaling between cell groups (now think of all the AAS orals in questions, being used,discontinued and reapplied), what People need to remember that hormones are "chemical messengers" that rely on "CONTINUES" messages/instructions to cells that display specific receptors for each hormone and respond to the signaling..Depending on the compounds and the individuals metabolization ratio the hormone can/may make changes directly to a cell, by changing the genes that are activated (now initiating a response, only to stop and cut it short, for what real reason???), or by making changes indirectly to a cell by stimulating other signaling pathways inside a specific cell group that is effected and effect other processes, thus this can "initiate" an intracellular cascade of events, a slew of unwanted side effects and so on.. So, the notion to utilize orals for a short duration, discontinue and apply a completely different targeting compound will induce imbalance within the endocrine system, within the internal network and switches that are attempting to find homeostasis which represents the body's love of static systems within the body (regulations/rule and order). This applies for the CNS, muscle, fat, hormones, neurotransmitters and brain secretions, as everything needs to be seen within a narrow range. The body has checks and balances, there are many systems of checks and balances in the body. If one fails, there is usually another one which can pick up the slack, and when one level goes up, so will an other, this is all part of homeostasis, but to initiate a war intrancelluar with misfiring, activation, deactivation, awakenings and canalization will only yield a slew of unwanted side effects.. What's the reasons and target purpose? Gains? These " Anabolic Erudite wannabes" from numerous internet panels fail to make mention of blood work, RBC, and BP related issues, or the mechanisms and nuero activation and secretion desensitization? How about a PCT for such a Frankenstein oral stack? What's the long term goals, sides, and potentials... Smoke and mirrors with nothing but just a "new" designer bro stack supported with no actually finds to support its benefits" Absurd, DANGEROUS, and if anyone considers such protocol from a half wit who gave you a piece of his mind, and you held on to it than I'm sure a demitasse would fit his head like a sombrero. And if anyone believes what these crafty entrepreneurs with their million dollar ideas by promoting innovative concepts that seem attractive, but yet possess no clinical data to support short and long term benefits are effective, you might as well stand side by side with them farting peas at the moon!
End result:
Continuous intake of AAS or any therapeutic drugs involves measuring drug concentrations in plasma, serum or blood that will achieve desired effects This information is real life clinical supported text book findings, in which is used to individualist dosage so that drug concentrations can be maintained within a target range, while being fully optimal with its instructions and designed pathways ways and actions..
Drug concentration can NOT be disrupted, and repeated, expecting same or more pronounced effects and the blood plasma needs to build again and again, yielding more stress on the liver, in lieu of being counter productive attempting to hinder liver toxicity... If bloods are routinely measured post-workout,port meal,pro-sup intake, one will see an extreme increase in liver functions aside from AAS used, but attempting to achieve desired or limited adverse effects from orals may correlate better with plasma or blood concentrations than they do with dose that is steady, rather than sporadic, or irregular intervals, ineffective short intakes,and discontinuation and re-administration. Now for these AAS in questions, the positive concentration measurements are a valuable surrogate of daily drug exposure especially to the Androgen receptors which are almost found throughout cellular groups allover the system, as well as FAT and muscle cell/groups, now in-order to initiate a positive nitrogen balance and satellite cell recruitment as well as steady and stable IFG-1 serums by achieving a steady stable/saturated response on AR's in muscle cells to promote size/growth, these AAS orals need continuous supply to keep the blood serum/medium within at the operative ranges and signaling and the same gives for other cellular cascade effects on other cells and AR's or outside the AR's
There's is simply no therapeutically value for athletes and none can be measured when it concerns the pharmacokinetic of these compounds or these protocol variation, individualizing this unorthodox drug dosage, it's difficult for me or anyone that possess some keen understanding on it's actually potentials are.,this is particularly relevant for drugs with a narrow target range or concentration-dependent pharmacokinetics and makes zero sense. Keep in mind that similarly, the variations and effects that are trying to be achieved here can be achieve over time within an individual and results and occur over time for a range of reasons with these drugs drugs using a "SAFER" continuous PROTOCOL, long as there remains a positive blood serum..If not, the agent will loss all effectiveness each time it's started over!
Therapeutic drug behavior is measuring threw drug serum concentrations, not some fancy innovated concept with no backing..
The consequences are seriously and should be placed in to great question by anyway of interpretation of the result in which this is "founded" and by whom made claims that it may produce desirable results without a slew of problems. This requires vast amount knowledge in pharmacokinetics and not something that has been spouted forum or regurgitated a thousands times over.
There's an abundance of clinical research and peer-reviewed data that strongly supports everything I'm advocated